


Post by EchelonHunt on May 17, 2015 20:02:51 GMT 8
Top Surgery Information & Techniques:
Top surgery is where a skilled surgeon reconstructs a female chest into a male chest, this may involve removing breast and fatty tissue with a scalpel or liposuction. The areolar is resized and if the nipples are large, they are trimmed down to a smaller size before being grafted back onto the person's new chest. Drains are put into the cavity of where the breasts once were to remove any build-up of blood. They are usually removed at your first post-op appointment, a week after surgery if all is well.
Being at your optimal weight for your body is highly ideal as the surgery results will be more satisfactory.
Keyhole technique:
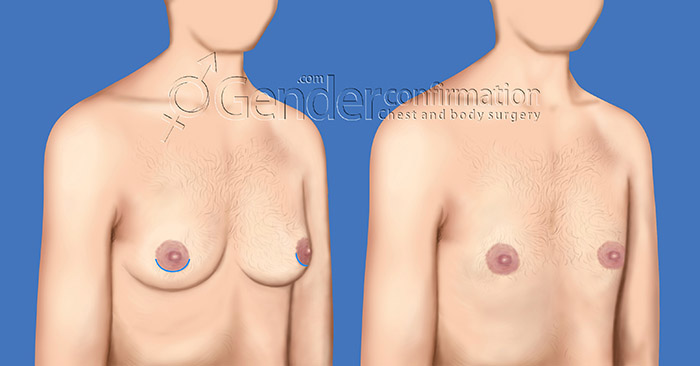
"A keyhole incision is ideal for patients with small breasts and good skin elasticity.
During this technique, a small incision is made under or across the lower border of the areola (the pigmented skin around the nipple).
A keyhole incision can remove underlying tissue, but it cannot address excess skin."
Trans-areolar incision with nipple reduction technique:
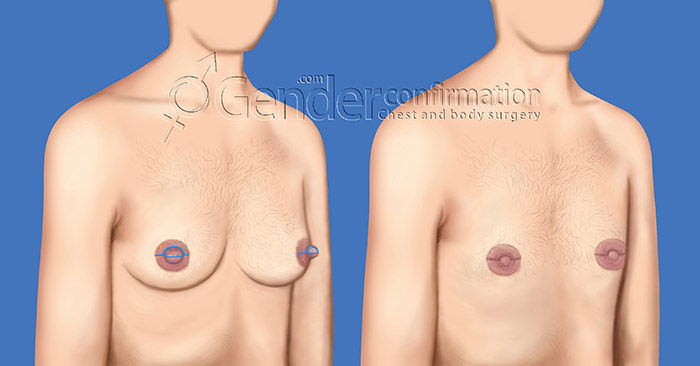
"This is in many ways very similar to the keyhole incision, except that it also incorporates a nipple reduction through a partial removal of nipple tissue, followed by folding the residual nipple over to reduce projection.
As with the keyhole incision, the incision length is minimal and well-hidden, but no extra skin can be removed through this approach."
Circumareolar technique:
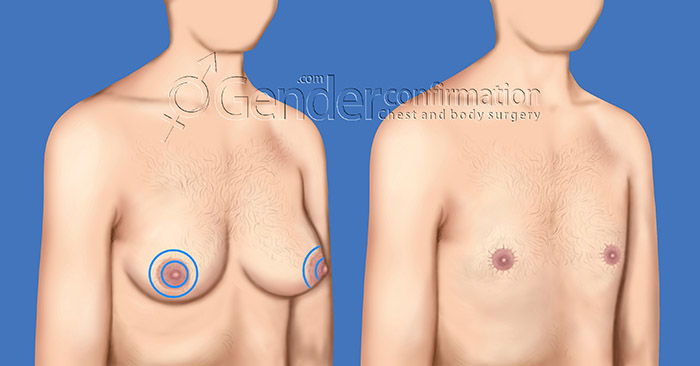
"A circumareolar incision is ideal for patients with moderate cup sizes and good skin elasticity.
A circular incision is made all the way around the edge of the areola to remove breast tissue.
A slightly larger ring incision is then made to remove excess skin.
The skin is pulled taut toward the center and the nipple is reattached to cover the opening.
This effect mimics the act of pulling a drawstring bag closed.
Another vertical incision that extends below the areola may also be necessary to target additional excess skin."
Fishmouth technique:
"This approach has been mentioned more recently, but is in fact infrequently used.
This approach has been thought to produce incision contours that are higher on the chest, and therefore perhaps more consistent with the border of the chest muscle.
However, it requires the final areolar position to be in line with the scar, which is not a natural proportion between the areola and the shadow of the muscle, which this scar is trying to mimic."
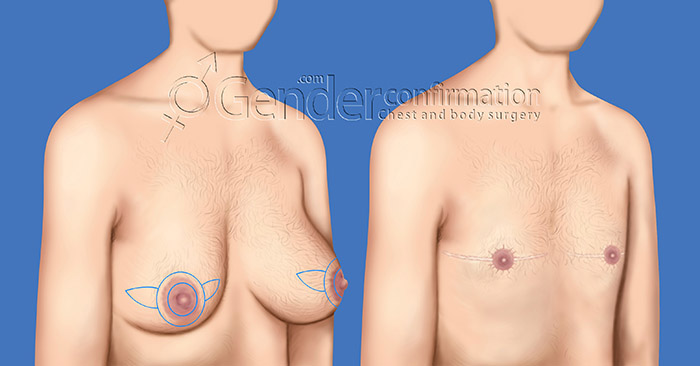
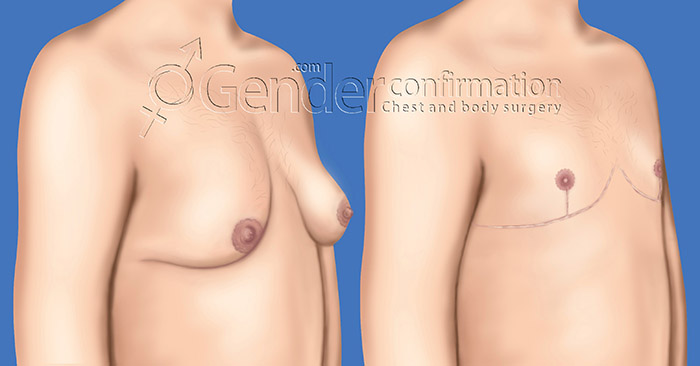
Double Incision technique:
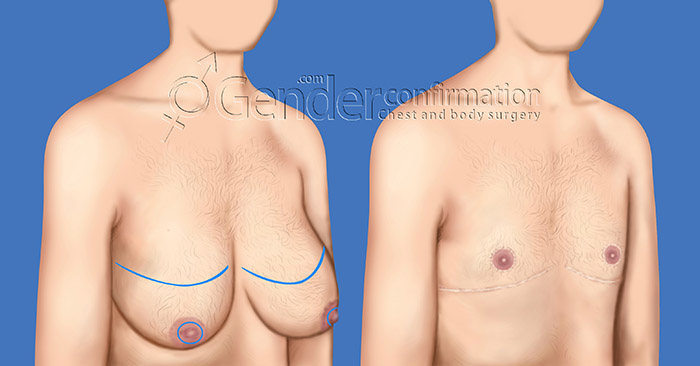
"A double incision pattern is usually needed for patients with large breasts, or breasts that exhibit a large degree of sagging.
A horizontal or U-shaped incision is made on the lower border of the pectoral is muscle (chest muscle).
The skin is peeled back so that breast and fatty tissue can be removed. Another incision is then made to remove the nipple.
Each nipple is resized, if necessary and then replaced as a free nipple graft in position that will give the chest a more masculine exterior.
If your breasts are shaped such that your nipple position is lower than the fold beneath the breasts, then you will likely require the double incision or an inverted T / anchor incision type."
Inverted T (anchor) technique:
"An inverted T (anchor) incision pattern is also an option for patients with larger breasts with extra skin.
This procedure keeps the nipple and areola attached to native body tissue, avoiding the need for a free nipple graft.
The surgeon does have good control over breast volume, but there is still a good chance that nipple sensation will be significantly diminished or need to recover from being numb.
Advantages are avoiding the free nipple graft (and therefore a lower risk of complete nipple loss) and having a nipple / areola that is more full & normal in appearance.
A disadvantage is the presence of an additional vertical incision, and there will not be quite as much flatness as with the double incision approach (because of the tissue left behind to supply blood to the nipple area)."
(Source & Citation: www.genderconfirmation.com/surgical-techniques/ )
Top surgery is where a skilled surgeon reconstructs a female chest into a male chest, this may involve removing breast and fatty tissue with a scalpel or liposuction. The areolar is resized and if the nipples are large, they are trimmed down to a smaller size before being grafted back onto the person's new chest. Drains are put into the cavity of where the breasts once were to remove any build-up of blood. They are usually removed at your first post-op appointment, a week after surgery if all is well.
Being at your optimal weight for your body is highly ideal as the surgery results will be more satisfactory.
Keyhole technique:
"A keyhole incision is ideal for patients with small breasts and good skin elasticity.
During this technique, a small incision is made under or across the lower border of the areola (the pigmented skin around the nipple).
A keyhole incision can remove underlying tissue, but it cannot address excess skin."
Trans-areolar incision with nipple reduction technique:
"This is in many ways very similar to the keyhole incision, except that it also incorporates a nipple reduction through a partial removal of nipple tissue, followed by folding the residual nipple over to reduce projection.
As with the keyhole incision, the incision length is minimal and well-hidden, but no extra skin can be removed through this approach."
Circumareolar technique:
"A circumareolar incision is ideal for patients with moderate cup sizes and good skin elasticity.
A circular incision is made all the way around the edge of the areola to remove breast tissue.
A slightly larger ring incision is then made to remove excess skin.
The skin is pulled taut toward the center and the nipple is reattached to cover the opening.
This effect mimics the act of pulling a drawstring bag closed.
Another vertical incision that extends below the areola may also be necessary to target additional excess skin."
Fishmouth technique:
"This approach has been mentioned more recently, but is in fact infrequently used.
This approach has been thought to produce incision contours that are higher on the chest, and therefore perhaps more consistent with the border of the chest muscle.
However, it requires the final areolar position to be in line with the scar, which is not a natural proportion between the areola and the shadow of the muscle, which this scar is trying to mimic."
Double Incision technique:
"A double incision pattern is usually needed for patients with large breasts, or breasts that exhibit a large degree of sagging.
A horizontal or U-shaped incision is made on the lower border of the pectoral is muscle (chest muscle).
The skin is peeled back so that breast and fatty tissue can be removed. Another incision is then made to remove the nipple.
Each nipple is resized, if necessary and then replaced as a free nipple graft in position that will give the chest a more masculine exterior.
If your breasts are shaped such that your nipple position is lower than the fold beneath the breasts, then you will likely require the double incision or an inverted T / anchor incision type."
Inverted T (anchor) technique:
"An inverted T (anchor) incision pattern is also an option for patients with larger breasts with extra skin.
This procedure keeps the nipple and areola attached to native body tissue, avoiding the need for a free nipple graft.
The surgeon does have good control over breast volume, but there is still a good chance that nipple sensation will be significantly diminished or need to recover from being numb.
Advantages are avoiding the free nipple graft (and therefore a lower risk of complete nipple loss) and having a nipple / areola that is more full & normal in appearance.
A disadvantage is the presence of an additional vertical incision, and there will not be quite as much flatness as with the double incision approach (because of the tissue left behind to supply blood to the nipple area)."
(Source & Citation: www.genderconfirmation.com/surgical-techniques/ )